【罂粟摘要】肺不张与术后肺炎的发生有关吗?一项单中心的回顾性研究
肺不张与术后肺炎的发生有关吗?一项单中心的回顾性研究
贵州医科大学 麻醉与心脏电生理课题组
翻 译:张中伟 编 辑:柏雪 审 校:曹莹
目的:肺不张在肺炎的发生发展中可能起到重要作用。然而,肺炎从来没有被认为是外科患者肺不张的结果。我们的目的是确定肺不张是否与术后肺炎的发生风险增加、重症监护病房(ICU)的转入和停留时间(LOS)有关。
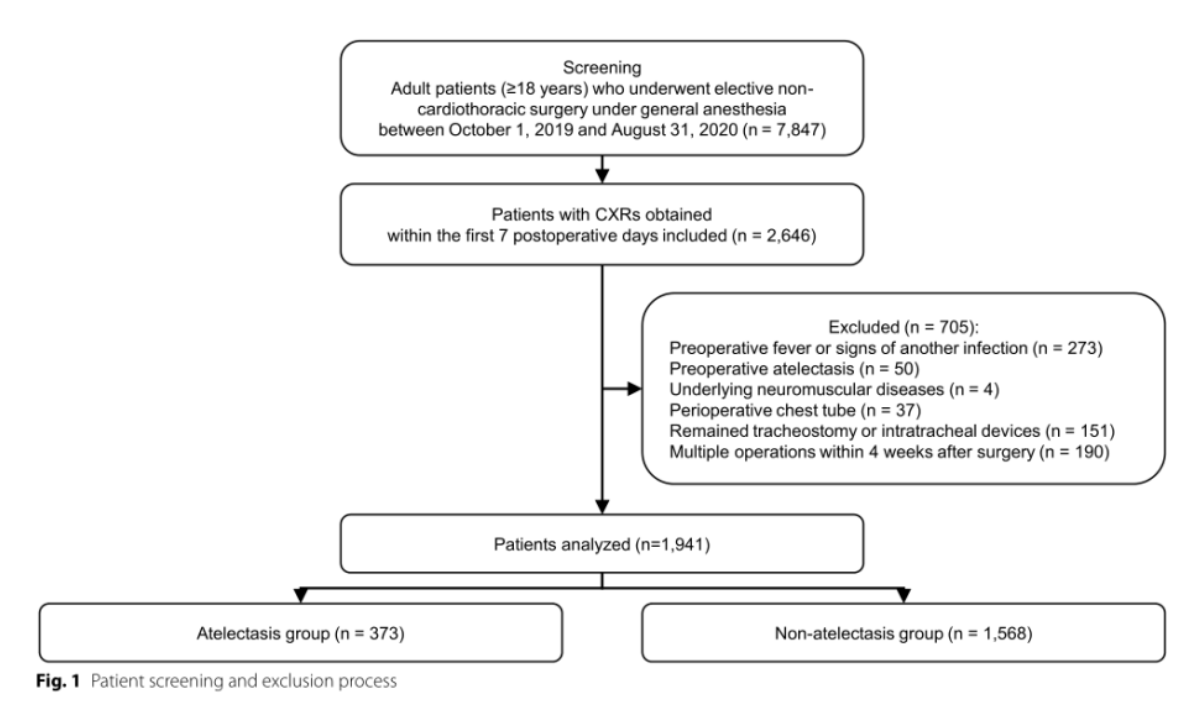
方法:本研究回顾了2019年10月至2020年8月期间在全身麻醉下接受择期非心胸手术的成人患者的电子病历。他们被分成两组:一组术后出现肺不张(肺不张组),另一组没有发生肺不张(非肺不张组)。主要观察指标是术后30天内肺炎的发生率。次要观察指标为ICU转入率和停留时间。
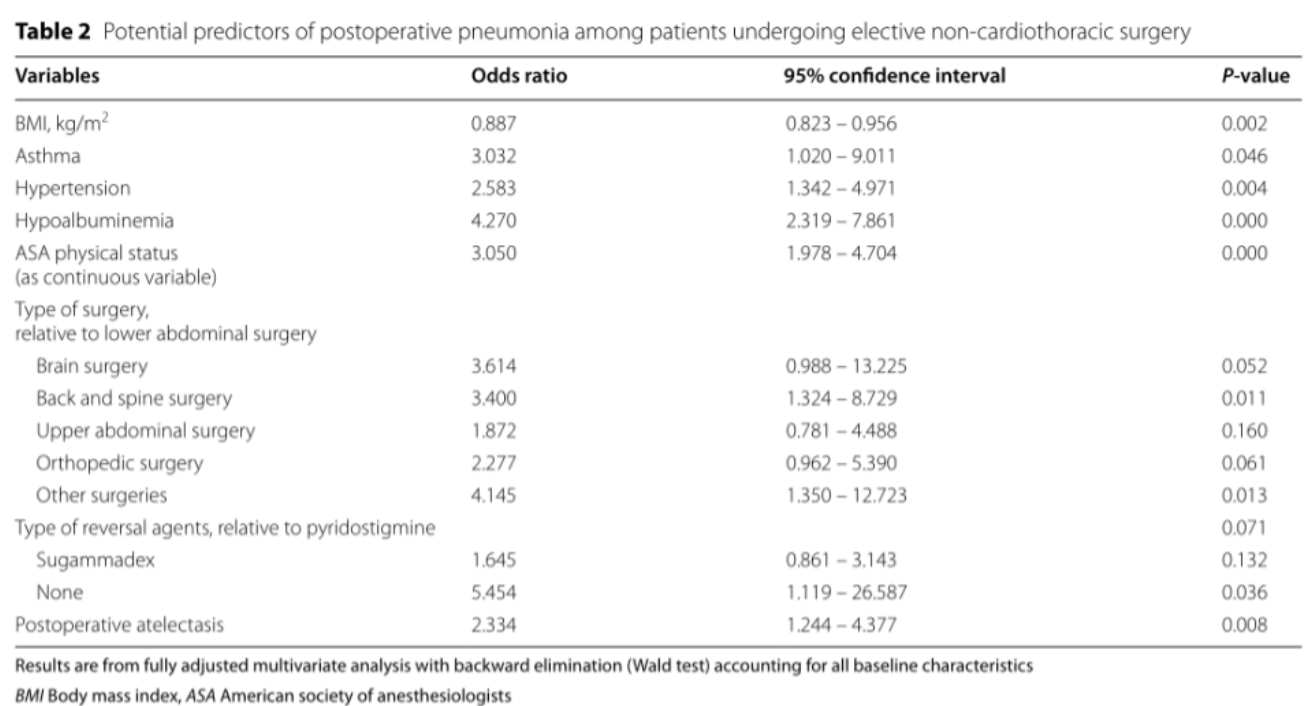
结果:与非肺不张组相比,肺不张组患者发生术后肺炎的危险因素更多,包括年龄、体重指数、高血压或糖尿病病史和手术时间。术后并发肺炎63例(3.2%),肺不张组为5.1%,非肺不张组为2.8%(P=0.025)。在多变量分析中,肺不张与肺炎风险增加相关(调整后的优势比,2.33;95%CI:1.24-4.38;P=0.008)。肺不张组术后中位LOS(7[四分位数范围:5~10天])明显长于非肺不张组(6[3~8]天)(P<0.001)。肺不张组调整后的中位LOS延长2.19天(β,2.19;95%CI:0.821~2.834;P<0.001)。肺不张组ICU住院率较高(12.1%vs.6.5%,P<0.001),但调整混杂因素后,两组间差异无统计学意义(调整后优势比1.52;95%CI:0.88~2.62;P=0.134)。
结论:在接受择期非心胸手术的患者中,术后有肺不张的患者肺炎发生率是无肺不张患者的2.33倍,LOS较无肺不张患者长。这一发现提醒医生们需要谨慎处理围手术期肺不张,以预防或减少包括肺炎和住院负担在内的不良事件。
原始文献来源:Eunji Ko, Kyung Yeon Yoo, Choon Hak Lim,et al.Is atelectasis related to the development of postoperative pneumonia? a retrospective single center study.[J]. BMC Anesthesiology (2023) 23:77
英文原文:
Is atelectasis related to the development of postoperative pneumonia? a retrospective single center study
Abstract
Background Atelectasis may play a substantial role in the development of pneumonia. However, pneumonia has never been evaluated as an outcome of atelectasis in surgical patients. We aimed to determine whether atelectasis is related to an increased risk of postoperative pneumonia, intensive care unit (ICU) admission and hospital length of stay (LOS).
Methods The electronic medical records of adult patients who underwent elective non-cardiothoracic surgery under general anesthesia between October 2019 and August 2020 were reviewed. They were divided into two groups: one who developed postoperative atelectasis (atelectasis group) and the other who did not (non-atelectasis group). The primary outcome was the incidence of pneumonia within 30 days after the surgery. The secondary outcomes were ICU admission rate and postoperative LOS.
Results Patients in the atelectasis group were more likely to have risk factors for postoperative pneumonia including age, body mass index, a history of hypertension or diabetes mellitus and duration of surgery, compared with those in the non-atelectasis. Among 1,941 patients, 63 (3.2%) developed postoperative pneumonia; 5.1% in the atelectasis group and 2.8% in the non-atelectasis (P = 0.025). In multivariable analysis, atelectasis was associated with an increased risk of pneumonia (adjusted odds ratio, 2.33; 95% CI: 1.24 – 4.38; P = 0.008). Median postoperative LOS was significantly longer in the atelectasis group (7 [interquartile range: 5–10 days]) than in the non-atelectasis (6 [3–8] days) (P < 0.001). Adjusted median duration was also 2.19 days longer in the atelectasis group (β, 2.19; 95% CI: 0.821 – 2.834; P < 0.001). ICU admission rate was higher in the atelectasis group (12.1% vs. 6.5%; P < 0.001), but it did not differ between the groups after adjustment for confounders (adjusted odds ratio, 1.52; 95% CI: 0.88 – 2.62; P = 0.134).
Conclusion Among patients undergoing elective non-cardiothoracic surgery, patients with postoperative atelectasis were associated with a 2.33-fold higher incidence of pneumonia and a longer LOS than those without atelectasis. This finding alerts the need for careful management of perioperative atelectasis to prevent or reduce the adverse events including pneumonia and the burden of hospitalizations.
END
来源 | 健康界
版权归原作者所有,若有违规、侵权请联系我们
- 1

